Why Communication Silos Kill Admissions Before They Start
When an admissions director tells you they spend half their day "checking status," they're describing a second, shadow job: manually stitching together a picture of reality that the system should already know.
This isn't a training problem. It's not a collaboration issue. It's an architectural failure.
The fragmented tools you're forced to use fragment the conversation before it begins.
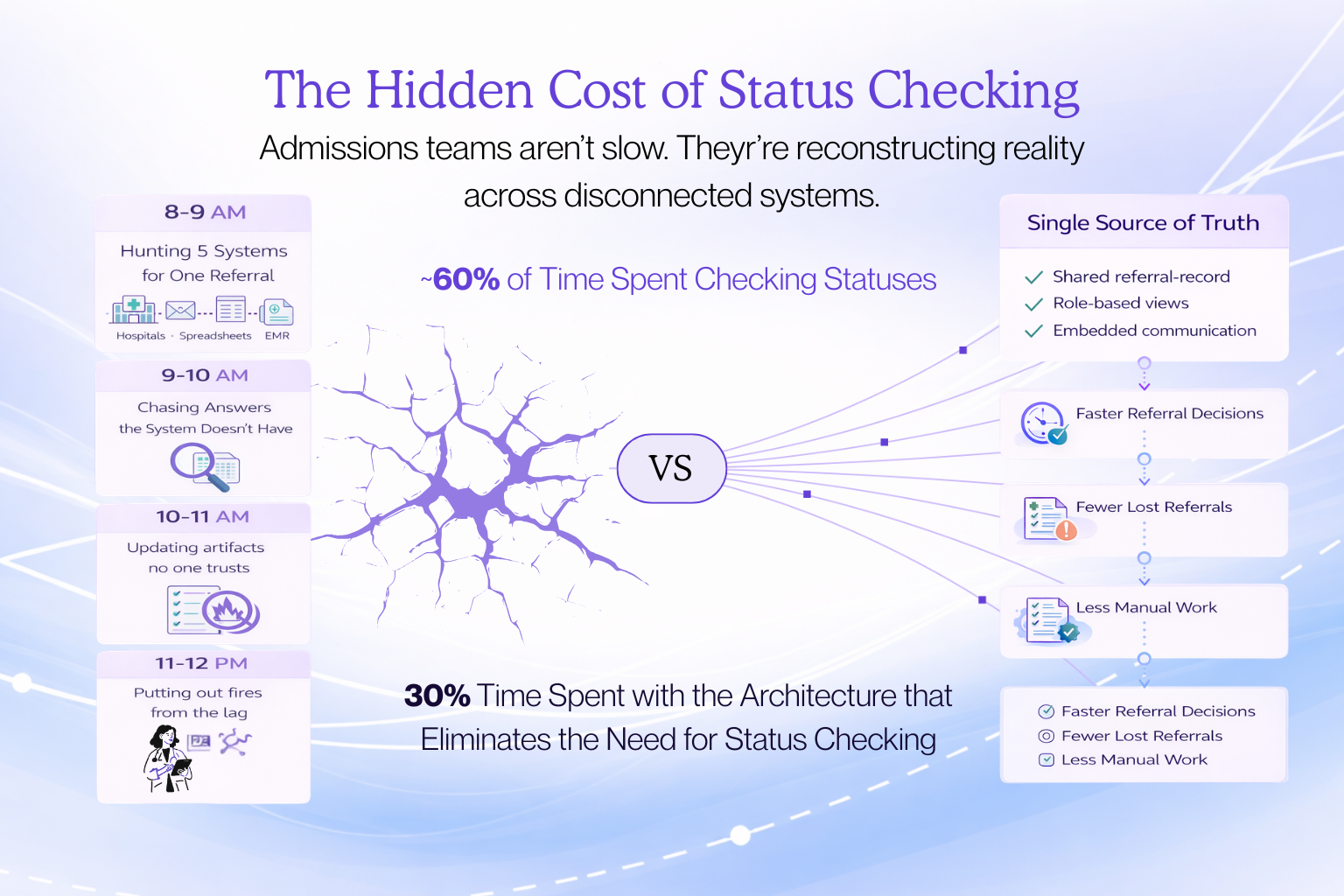
The Hidden Cost of "Status Checking"
The Morning Cycle
You log into hospital portals, check spreadsheets, search the EMR. You're reconciling three slightly-wrong versions of the truth just to answer: "Is this referral actually still alive?"
Chasing Answers
You scroll through emails and texts hunting for updates. You call intake staff, ping liaisons, and message case managers. Most of this time isn't moving referrals forward. You're reconstructing a story that should already be visible in one place.
Updating Systems No One Trusts
You edit spreadsheets, drop notes into the EMR duplicating what's in email, and prepare reports you know will be outdated by the time they're printed. "Checking status" means being the human ETL pipeline: extract from portals and people, transform into your best guess, load into the tools leadership sees.
Fighting Fires
You respond to angry calls from case managers, scramble to verify whether referrals were received, and reconcile discrepancies when patients show up but aren't on any "pending" report. You're not checking status. You're defending the integrity of a system you know is full of holes.
Why Organizations Tolerate This
Heroics are culturally rewarded. The director who stays late reconciling portals and spreadsheets is seen as dedicated, not misused. That heroism masks how broken the system really is.
Workarounds hide system failure. As long as humans patch gaps manually, the full cost never surfaces. Patients get admitted, metrics look "good enough," and teams solve today's problem rather than escalate the architectural issue.
Change feels riskier than pain. Rebuilding core workflows is disruptive and politically hard. Living with fragmented reality is painful but familiar.
People blame workload, not architecture. The story is "we're understaffed" not "our systems require humans to do what software should handle." That leads to hiring more coordinators instead of questioning why the manual work exists.
Digital solutions have burned them before. Clunky EHR rollouts created skepticism. It feels safer to lean on spreadsheets than bet on software that might not respect workflow.
The Three Communication Breakpoints That Cause Referrals To Stall
Breakpoint 1: Referral Source to Intake
Hospitals send referrals through portals, faxes, emails, and phone calls. Each channel creates its own version of the patient story. Providers require as high as 4.23 full-time equivalent staff per physician for handling paperwork alone.
Breakpoint 2: Intake to Clinical Review
Intake emails a PDF to a shared "clinical review" inbox. In their spreadsheet, they flip status to "Sent to clinical." From their perspective, the handoff is done.
Architecturally, nothing changed. There is no system state called "in clinical review," no owner field updated, no task created. A file moved. The referral record did not.
The shared inbox becomes the bottleneck. The clinical nurse faces 200+ unread messages. They triage by subject line. If the email came in late Friday or has a vague subject, it's invisible.
Multiple "sources of truth" drift out of sync. Intake's spreadsheet shows "clinical review." Clinical's notebook doesn't list the patient because they never saw the email. The EMR shows nothing.
Breakpoint 3: Clinical to Finance/Operations
Clinical says "yes," then finance discovers the payer won't cover it, or ops realizes there's no bed. This happens because the clinical decision was made without real-time visibility into payer status, authorization requirements, or capacity constraints.
Most systems have leakage rates of more than 50 percent.
Best Practice: Single Source of Truth Architecture
The solution isn't better communication training. It's designing systems where the right information reaches the right person at the right moment without anyone having to ask.
Shared queues eliminate the need for status updates. When every referral's journey is visible to all stakeholders in one platform, you stop playing telephone. Referral sources, intake teams, clinical reviewers, finance, and operations all see the same real-time picture.
State changes on the referral, not in someone's inbox. When intake clicks "send to clinical," the system commits a state change on a single referral object. That state change happens on one canonical referral record in the database, not in a spreadsheet row or an email subject line.
The system will not allow a "clinical review" state without required fields. What lands with clinical is structured and complete enough to act on.
Ownership is reassigned explicitly. As part of that transition, the primary owner is reassigned from an intake user to a clinical role or named clinician, based on routing rules. That ownership change is recorded as an event: "Owner changed from Intake Queue to RN_Clinical_Team_A at 10:14 a.m."
There is always exactly one "who owns this now," and the system controls it.
Best Practice: Role-Based Context Without Role-Based Silos
Different stakeholders need different views of the same referral, but they shouldn't be working in different systems.
Clinical reviewers see clinical context. Concise clinical summaries, problem lists, medications, functional status, and risk factors.
Finance teams see financial context. Plan details, prior authorizations, and estimated reimbursement.
Operations sees capacity context. Bed and capacity data so "no bed" isn't a surprise after clinical says yes.
Everyone looks at the same referral object through different lenses. The conversation stays unified.
Best Practice: Embedded Communication That Lives With The Referral
Internal notes stay attached to the referral. All communication is logged on the referral itself, not split across email threads.
Requests become tasks. "Need latest labs" becomes a task with due time and ownership, not a loose email reply.
Best Practice: Transparent Decision Trails
Explicit logging. Each decision traces to specific criteria, inputs, and actions: who reviewed what, when, and under what rules.
Override tracking. Deviations from default rules are recorded with reasons, transforming friction into learnable data.
Specific denial reasons. Not "not a fit" but specific clinical, operational, financial, or capacity explanations.
The Measurable Impact
Closed-loop completion rate jumps. The share of referrals that end with a definitive, system-recorded outcome increases because referrals can't quietly die in "pending" anymore. Every referral must go somewhere in the state machine.
Referral-to-decision time drops. Median time from referral received to clear yes/no often drops by days because the system is always pushing the next action instead of waiting for humans to remember.
Conversion rate on real referrals climbs. As leakage shrinks and follow-up becomes consistent, you convert more of what you already get without needing more leads.
Manual touch and rework falls. The number of calls and emails per referral drops because status lives in one place, and tasks are system-driven. Directors stop being human ETL just to know what's going on.
What Becomes Visible For The First Time
Leakage by stage. See exactly where referrals are lost: intake, clinical review, financial clearance, capacity, or patient decision.
Bottlenecks. Financial clearance adding 3 days, certain hospitals sitting in "no response" for a week.
Real demand vs. visible census. All clinically appropriate referrals you could have taken vs. actual admits.
Exception patterns. How often you bypass normal rules, for which partners and payers, with what impact.
Partner and payer performance. Who sends clean referrals vs. who generates friction.
The "Oh, This Is Real" Moment
The morning where nothing is "off-list." Every referral from every source is already in one queue, deduped, with owners and next steps. The board on the screen is the work. You're not asking "What are we missing?" You're deciding "What should we do first?"
The fire that doesn't require a hero. A hospital calls about a referral. Instead of scrambling through email, you type the name, see the current state and owner, and answer in one sentence. You resolved a high-pressure moment without being a human ETL pipeline.
The meeting where the arguments stop. Someone asks "Why are we missing census?" Instead of anecdotes, you pull up data: 23% died waiting for auth, 15% at capacity, time to first touch dropped from 2 days to 6 hours. The room shifts from opinion to system.
From Remembering Everything to Improving Something
The real transformation is when your value moves from remembering everything to improving something.
When the system finally remembers for you, you stop seeing the platform as another tool to feed. You start seeing it as the central platform that lets you do the job you were actually hired to do.
Communication silos aren't a people problem. They're an architectural failure.
The solution isn't more meetings, more training, or more heroics. It's designing systems where the right architecture makes silos structurally impossible rather than culturally discouraged.
When you build that architecture, you don't just improve communication. You eliminate the need for most of it.
References and Further Reading
On Healthcare Workarounds and System Fragmentation:
- Pennsylvania Patient Safety Authority - Workarounds in Healthcare
- AHRQ PSNet - Workarounds and Resiliency on the Front Lines of Health Care
- Administrative Burden in Healthcare: The Impact on Physician Workload
- JMIR Human Factors - Workarounds in Electronic Health Record Systems
On Referral Management and Communication Breakdowns:
- Communication Failures in Healthcare Referral Systems
- Breaking the Bottleneck: Fixing the Referral Crisis
- Referral Intake vs. Referral Management: Understanding the Difference
- Addressing Patient Referral Leakage in Healthcare Systems
On Closed-Loop Referral Management:
- Closed-Loop Communication and Patient Safety
- Understanding and Preventing Referral Leakage
- Complete Guide to Closed-Loop Referrals
- How Referral Systems Are Transforming Healthcare
On Healthcare Workflow Automation:
- Healthcare Workflow Automation and EHR Optimization
- How Automating Clinical Workflows Improves Patient Experience
- Clinical vs. Administrative Workflow Automation
On AI in Healthcare and Clinical Decision Support:
- AI-Assisted Clinical Decision Making: Opportunities and Challenges
- Human-in-the-Loop AI Systems in Healthcare
- Automation Bias in Clinical Settings
- Optimizing Referral Management with AI
On Healthcare Tracking and Metrics:
- Best Practices for Referral Tracking in Healthcare
- How to Measure New Patient Conversion Rates
- Healthcare Referral Management: A Comprehensive Guide
About Careflow:
- Careflow - Central Hub for Healthcare Admissions
- Careflow CRM Platform Overview
- Careflow CRM in the Healthcare AI Database
.png?width=352&name=PR%201%20Image%20(1).png)

.png?width=352&name=AE%20Content%20Round%202%20(2).png)
